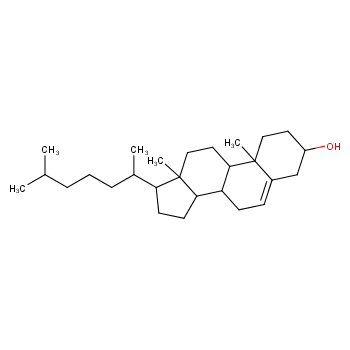
Cholesterol is a soft, waxy substance categorized as a steroidal alcohol or sterol. As the predominant steroid in the human body, it serves as a fundamental component within every cell. Essential to life, cholesterol is present in most animals and many plant species. The biosynthesis of cholesterol primarily takes place in the liver, although other organs may also contribute to its production. Various important substances, such as vitamin D, steroid hormones (including sex hormones), and bile salts, are synthesized from cholesterol. Predominantly located in cell membranes, cholesterol plays a vital role in cellular structure.
The discovery of cholesterol dates back to 1769 when Poulletier de la Salle (1719–1787) isolated the compound from bile and gallstones. Michel Eugène Chevreul (1786–1889) rediscovered it in 1815, naming it cholesterine. The term originates from the Greek words "khole," meaning bile, and "steros," meaning solid or stiff. The suffix "ine" was later modified to "ol" to denote its classification as an alcohol.
Humans produce approximately 1 gram of cholesterol daily in the liver, while dietary cholesterol is obtained through food consumption. High-cholesterol foods are linked to saturated fats and trans-fatty acids (commonly referred to as trans fats). Dietary cholesterol is predominantly found in animal products, such as meats and dairy items. Table provides information on the cholesterol content in various common foods.
Cholesterol is commonly associated with cardiovascular disease, and its routine measurement is employed to assess potential health risks. Elevated blood serum cholesterol levels often correlate with excessive plaque deposits in the arteries, a condition referred to as atherosclerosis or arterial hardening. While high total blood cholesterol levels are linked to heart disease, it is crucial to differentiate between cholesterol types when interpreting these levels. Cholesterol is categorized as "good" or "bad" based on its physiological role, which is determined by the associated lipoproteins.
Low-density lipoprotein cholesterol (LDL cholesterol) is commonly known as "bad" cholesterol, while high-density lipoprotein (HDL) is termed "good" cholesterol. Understanding the distinction between LDL and HDL cholesterol requires insight into the substances associated with cholesterol in the body. Cholesterol, being a lipid, exhibits low solubility in water and blood. To facilitate the delivery of cholesterol synthesized in the liver to the rest of the body, lipoproteins, acting as carriers for cholesterol and triglycerides, are manufactured by the liver. Lipoproteins are biochemical assemblages of fat and protein molecules, with various types present in human blood.
Cholesterol leaves the liver as very-low-density lipoprotein (VLDL), characterized by a high percentage (50–65%) of triglycerides and a relatively low protein composition of 10% or less. The density of lipoproteins is dictated by the percentage of fat and protein, with higher protein content resulting in greater density. As VLDL circulates through the bloodstream, encountering the enzyme lipoprotein lipase in organ capillaries, triglycerides are delivered to cells for energy utilization or storage as fat. Depletion of triglycerides transforms VLDL into intermediate density lipoprotein (IDL), which, in turn, converts to LDL in the presence of LDL receptors binding to apolipoprotein Apo B-100. LDL cholesterol, delivered to tissues by Apo B-100, has the propensity to adhere to blood vessel walls, hindering blood flow and potentially forming plaque, contributing to atherosclerosis.
Atherosclerosis occurs when excess cholesterol, along with other substances such as fats, lignin, and calcium, combines to form hard deposits on the inner lining of blood vessels. LDL cholesterol is labeled as "bad" cholesterol due to its association with these issues. In contrast, HDL is produced in various tissues, including the liver and intestines, and is characterized by low triglyceride levels and high protein content (approximately 50%). HDL, or "good" cholesterol, transports cholesterol in the bloodstream back to the liver for breakdown and excretion. While a definitive reduction in heart disease risk has not been conclusively demonstrated with high HDL levels, an inverse relationship between HDL and heart disease exists.
Maintaining an optimal balance of cholesterol in the bloodstream necessitates a sufficient presence of receptors to effectively process cholesterol levels. These receptors undergo continuous regeneration, production, and elimination within cells, responding to blood biochemistry. The liver harbors the highest concentration of these receptors. Inadequate receptor numbers or an excessive intake of dietary cholesterol can result in elevated blood cholesterol levels. Familial hypercholesterolemia, a genetic disorder, arises when an individual inherits a defective gene, hampering receptor production. Excessive dietary cholesterol inhibits LDL receptor production, contributing to heightened blood cholesterol and Apo B.
Routine lipid screening for cardiovascular risk assesses total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides, reported in milligrams per deciliter of blood (mg/dL). Interpretation of recommended cholesterol levels must be judicious, considering individual risk factors. The National Center for Cholesterol Education (NCEP), endorsed by the American Heart Association, emphasizes LDL as the primary determinant for therapeutic decisions. For those with no more than one risk factor, an LDL less than 160 mg/dL is recommended, while individuals with coronary heart disease should target less than 100 mg/dL. NCEP designates HDL below 40 mg/dL as low, constituting 20–30% of blood cholesterol, and considers a triglyceride level below 150 mg/dL as normal.
Heart disease, the leading cause of death in adults over 35 in the United States, necessitates comprehensive strategies to mitigate cholesterol's impact. Principal approaches include dietary modifications, lifestyle adjustments, and pharmaceutical interventions. Dietary changes involve reducing saturated and trans-fats, with trans-fats adversely affecting both LDL and HDL cholesterol. The FDA mandated trans-fat disclosure on nutritional labels from January 1, 2006. Soluble fiber-rich foods, omega-3 fatty acids, and lifestyle changes such as exercise, smoking cessation, and weight management contribute to cholesterol control.
Over the past two decades, the advent of statin drugs has transformed heart disease treatment. Statins inhibit HMG-CoA reductase, a key enzyme in cholesterol biosynthesis. HMG-CoA converts to mevalonate during cholesterol synthesis, and statins mimic this structure. Leading statins, such as lovastatin (Mevacor), atorvastatin (Lipitor), and simvastatin (Zocor), have become top-selling drugs globally. Lipitor, for instance, achieved approximately $13 billion in annual sales in 2005, underscoring the significant impact of statins in heart disease management.
Richard L. Myers (2009). The 100 Most Important Chemical Compounds: A Reference Guide. Greenwood Publishing Group. October 1, 2009. https://doi.org/10.1021/ed086p1182
 |
|